Endoscopic thoracic sympathectomy (ETS) surgery is made out to be a safe procedure on most surgeons' websites with typical short-term dissatisfaction rates for hand sweating patients quoted as being less than five percent. From my years of experiences of having: talked to or e-mailed a large number of ETS patients; reading personal blogs and websites on the web regarding this subject; and checking out forums and reddit threads from people who underwent this surgery; the dissatisfaction rate is significantly higher in the long run. The biggest reason is due to the side effect of compensatory sweating (CS), though most surgeons do not divulge a number of changes to your body that can often occur in the longer term.
Your body will lose its ability to sweat above the nipple line when you have the surgery to stop your hand sweating. Some surgeons forget to mention this phenomenon. I got this side effect after my ETS surgery in 1998 to cure my sweaty palms. However, it has luckily not affected me adversely as far as my upper body becoming overheated when I play sports or walk a lot in hot weather. I do feel like my scalp is very dry sometimes, but perhaps that has nothing to do with my not sweating in that area. Some people have complained of a very dry face and scalp after ETS surgery. A few people have had major body temperature changes (thermoregulatory disturbances) after surgery during times of stress, and they have theorized this to be a result of an altered body "thermostat" that cannot enable heat loss via sweating through the upper body after surgery. I have been lucky and do not suffer from any of these problems.
Edit: Since around the mid-2000s, many surgeons have been cutting the T-3 and/or T-4 ganglions for palmar hyperhidrosis instead of the T-2 ganglion, and it seems like this side effect of upper body anhidrosis will not usually occur with the new surgery. However, some surgeons believe that cutting T-3 and/or T-4 to cure excessive hand sweating problems might lead to a higher likelihood of re-occurrence of palmar sweating. But the vast majority still seems to prefer this risk over cutting T-2. If you have both palmar and plantar hyperhidrosis, your surgeon might prefer doing the combined T-3+T-4 thoracic sympathectomy.
ETS reduces the resting heart rate in a fraction of patients. This fraction has been listed anywhere from one-tenth to well over one-half depending on which surgeon you listen to. My resting heart rate fell by around ten percent after my ETS surgery in 1998 per surgery documents, but later on might have gone back to normal as far as I can tell. Although probably not dangerous, this is something to keep in mind, and you should ask your surgeon about this if he/she forgets to mention it. Are you willing to mess with your heart rate to get rid of consistently sweaty palms? I would still say yes based on my terribly sweaty palms. The reason ETS reduces your heart rate is because some of the upper thoracic ganglions in the sympathetic chain have direct and/or indirect connections to the heart. It should be noted that the parasympathetic nervous system (the opposite of the sympathetic nervous system) also affects the heart rate. The sympathetic nervous system will raise your heart rate when you are in danger, and the parasympathetic nervous system lowers your heart rate.
Some surgeons are now warning that if you are an athlete, ETS might reduce your peak performance due to this side effect, but other surgeons say that ETS has no effect on your maximum heart rate. For me, a slightly lower heart rate (assuming that side effect was permanent) does not seem to have made any difference in athletic ability. My resting heart rate is never below 60 beats per minute, which is the cutoff point for bradycardia. Usually, problems can only arise if your heart rate falls below 50 beats per minute. Also, some surgeons have suggested that a slightly lower heart rate is good for you in the long run. Interestingly, many excellent athletes such as cyclists Lance Armstrong and Miguel Indurain have an excessively low resting heart rate of around 30 beats per minute. For most adults, resting heart rates fall between 60 and 80 beats per minute.
ETS leads to compensatory sweating aka compensatory hyperhidrosis (a better term is reflex sweating per Dr. Chien-Chi Lin) in a majority of patients. In the past, most surgeons usually estimated a figure of around 40-60 percent, but this figure has steadily increased as more and more patients have started getting compensatory hyperhidrosis a year or two after surgery and the surgeons have realized that the problem does not necessarily start the day after the surgery. This is especially true if the surgery is performed in winter, and the patient is thus unable to experience compensatory sweating at its worst in summer weather.
The palms and feet house most of the body's sweat glands, so it seems logical to infer that stopping sweating at either place will almost always guarantee compensatory sweating elsewhere. For me, the compensatory sweating occurred in my feet instead of in my chest or back or thigh areas as is most common. It is also possible that I started noticing my feet sweating more once the hand sweating was entirely eliminated.
Your feet sweating (aka plantar hyperhidrosis) can become worse than before surgery. Most people with palmar hyperhidrosis also have plantar hyperhidrosis. Surgeons typically say that there is anywhere from a 50-95 percent (depending on whom you listen to) chance of a reduction in feet sweating after ETS for palmar sweating (i.e., a bonus benefit). The feet sweating will remain the same as before ETS in the remaining patients according to the surgeons. However, I think that I have experienced an increase in feet sweating post ETS, though I am not absolutely 100% certain. Many others have reported a similar outcome of increased feet sweating. I haven't seen a single surgeon point out this possibility to date. Sweat signals to the feet generally come from the lumbar sympathetic chain in your lower back. So it seems that in some patients, the lumbar sympathetic chain starts transmitting more sweat signals to the feet once palmar sweating has ceased as a result of the destruction of part of the sympathetic (thoracic) nervous system. A lumbar sympathectomy can possibly cause reverse ejaculation in men and urinary incontinence in women (among other side effects), so almost no surgeon offers this procedure for the purposes of curing feet sweating anymore.
Edit: As of 2008/2009, it seems like lumbar sympathectomy is becoming fashionable again, although only one surgeon in the US currently offers it. I would hold off on getting this surgery until more results come in, and I would recommend trying iontophoresis on your feet if you have not already done so.
Edit: In May 2009, I finally got rid of my excess feet sweating using Hidrex iontophoresis. You must attempt iontophoresis therapy before looking into getting endoscopic thoracic sympathectomy surgery!
You can get extremely cold hands post ETS, and like some of the other side effects, this can show up a year or more after the surgery. So this side effect doesn't show up in most surgeons' list of potential side effects that is often based on surveys conducted in the immediate aftermath of surgery. This is also why ETS is not performed to cure Raynaud's (cold hands) syndrome by most surgeons anymore, since initially warm hands post-ETS can become extremely cold a year or two down the road. According to an e-mail to me from the pioneers of the endoscopic method of sympathectomy, Dr. Goran Claes and Dr. Christopher Drott, this severely cold hands side effect happened in two percent of their patients due to "increased sensitivity to surrounding catecholamines". I get this side effect once in a while during the peak of winter if I am not wearing gloves, and one or two of my fingers become pale white.
After ETS, some patients (typically less than five percent in the case of ETS for palmar sweating) experience a recurrence of their original symptoms. This type of recurrence is usually more common with regards to ETS for facial blushing, Raynaud's Syndrome and other such non-hyperhidrosis related problems. In my own case, I had very mild right hand sweating return a year or so after ETS while the left hand has always remained extremely dry. During intense exercise, my right hand can get a bit moist, but otherwise, it is always bone dry (even in 100F weather). It is unclear to the surgeons why this recurrence occurs, and some claim that there is no way a destroyed ganglion can regenerate, so the sweat signals must be transmitting via other pathways. Many patients need to get re-operated upon if the recurrence is significant, as was the case with a fellow American patient who was with me when I had my ETS surgery in Sweden in 1998. I am not sure how the re-operation works if the destroyed ganglion has not regenerated. Perhaps the thoracic surgeon destroys other nearby thoracic ganglions that were not destroyed originally (i.e., T-2 or T-3 or T-4) in the event of recurrence? He or her also has to navigate the surrounding scar tissue from the initial operation.
The only side effects that surgeons have discussed honestly and have quoted consistent risk percentages for are Horner's Syndrome (droopy eyelids) and Gustatory Sweating. Gustatory sweating (GS) is significant forehead sweating when eating or even smelling spicy food and can occur a year or two after ETS. Horner's Syndrome is extremely rare in the hands of an experienced surgeon, since it requires damage to the stellate ganglion (T-1). The few patients who do get permanent Horner's Syndrome then have to get cosmetic surgery to normalize their appearance. Gustatory Sweating occurs in anywhere from 10-20 percent of patients, although it is unclear if this figure is higher in the long run. I got the gustatory sweating side effect a year or two after surgery, but only when eating very spicy food, which I unfortunately enjoy. It is quite strange that I am unable to sweat at all from my forehead after having had T-2 ganglion endoscopic thoracic sympathectomy, even while exercising during 90 degree Fahrenheit temperatures. Yet the same forehead can sweat profusely when I am eating very spicy food.
Edit 2013: In recent years, my GS has become very rare and I actually look forward to getting it. I miss the sensation of not being able to sweat on my forehead when playing sports or when exerting myself in other ways. So when I eat very spicy food and once in a while get the sweat and moisture rolling across my forehead, I derive pleasure from it. I feel normal, and imagine that I am getting rid of waste and toxins via the sweat (although it seems like this is a myth).
Problems that can occur during surgery include pneumothorax, intercostal neuralgia, pleural effusion and even death on very rare occasions. It seems like around ten deaths have occurred in Western countries as a result of ETS surgeries. Pneumothorax entails a partial or full lung collapse after the operation. Intercostal neuralgia is localized pain in the chest wall area. Pleural effusion is the abnormal buildup of excess fluid in the lungs.
There are a host of other side effects that some people have complained about that are possible due to ETS such as sensitivity to light, dizziness, blood pressure changes, dry scalp, hair loss etc... If enough people complain about a specific problem and at least a few surgeons verify the problem as a side effect of ETS (as has been the case for all the side effects I listed above), I can add the problem in the above list. Otherwise, I am treating those rumored side effects as unrelated to ETS.
Until 2010 or so, a T-2 sympathectomy was the procedure of choice to cure hand sweating, facial sweating and facial blushing. The cut was a little higher for facial blushing (closer to T-1), but ultimately you stopped the signals arising from T-2 for all three of these conditions. In the more distant past, surgeons even cut T-2, T-3 and T-4 for hand sweating. Nowadays, most surgeons cut T-3 or T-4 to treat palmar hyperhidrosis. This seems to have reduced the most common side effect of compensatory sweating. It seems like more significant types of upper body nervous system signaling (including to the heart) arise from the upper portion of the thoracic cavity (i.e., T-1 and T-2).
Check out the portion of the website where I discuss the evolution of ETS surgery and confusion regarding so many different ETS techniques. Surgeons have managed to personalize their own variety of ETS, sometimes for marketing purposes. Some prefer cauterizing the nerves, others prefer clamping or clipping them, and a few try to still remove the entire ganglion. In the past, some placed a lot of emphasis on finding and destroying kuntz nerves, but this is not given as much importance these days. Some cut or clamp the ganglion at slightly different levels above the designated thoracic rib number. And some still prefer destroying T-2 to stop palmar hyperhidrosis, though seem to now prefer T-3 or T-4.
Many people make a very fast decision to have ETS. A quick 1-hour (30 minutes per side) minor surgical procedure that often doesn't even require overnight stay sounds miraculous. However, this surgery can sometimes lead to long-term turmoil on the internal networking of your body. After all, there must be an evolutionary reason as to why the sympathetic nerve chain is in a location where it can never be damaged unlike virtually all other components of your body. Humans can easily damage external parts of their bodies through physical injury. In addition, most internal organs such as the brain, heart, kidney, liver, and lung can be damaged by cancer, diet, drinking, drugs, smoking, pollution and more. However, to my knowledge, the sympathetic nervous system (or more specifically, the thoracic ganglions) can almost never be physically damaged without surgical intervention. This is because the ganglions are located deep inside the chest and made up in a rope like manner that cannot break easily. A bad diet, smoking, drinking and other such bad life choices cannot damage the sympathetic nervous system.
Having said all that, ETS is a last resort option that is almost a surefire cure for your palmar (and facial) hyperhidrosis. However, I firmly believe that there is an extremely strong chance of curing hyperhidrosis using one or a combination of the numerous alternative methods available that are outlined on this website (and discussed in the forums). But you have to be persistent with such treatments, while ETS when successful is a one-and-done solution.
If you have already had hyperhidrosis surgery and are still reading this page, I hope that I have not turned you into a hypochondriac who starts imagining that every possible physical problem you have is due to sympathetic nervous system destruction. Some medical problems and negative changes to your body could be part of aging or part of your genetic destiny. There are several sites out there that blame ETS surgery for every possible medical condition on earth, and they are even more damaging than the surgeons' sites that make it sound like ETS is an easy side effect free answer to your sweating problems.
Moreover, I have talked with a few happy people who had open surgical sympathectomy many decades ago to cure hyperhidrosis. They had numerous ganglions removed along with major bleeding and other significant trauma during and after the more extensive open surgery. These people are enjoying their life and old age despite the side effects they had to deal with all their lives. In the end, willpower can often overcome most side effects.
Update: June 26, 2023
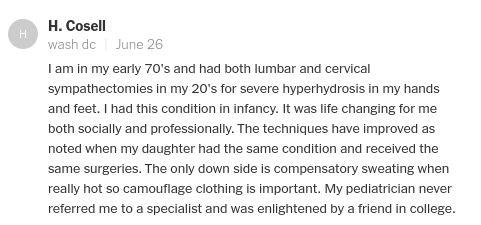
In a recent NY Times article about excessive sweating, the reader comments are especially interesting. I am pasting the screenshot of my favorite one below. This reader had both cervical and lumbar sympathectomies for his/her hand and feet sweating almost 50 years ago. Insane that in his/her early 70s, this person is still interested in the subject and posting an online newspaper comment. A cervical sympathecomy is in the neck region and even higher up than a thoracic sympathectomy. Perhaps they sometimes used to do the former decades ago for hyperhidrosis? Or this reviewer just got an incorrect name given to him/her? In any case, this just shows that you can live a normal life even decades after a highly invasive open sympathectomy with major and numerous ganglion destruction. Note that the cervical region vertebrae are labeled from C1-C7; the thoracic region goes from T1-T-12; and the lumbar region goes from L1-L5.